
IHE and openEHR
Integrating the Healthcare Enterprise (IHE) is an initiative by healthcare professionals and industry to improve how medical systems share information. Rather than creating new standards, IHE promotes the coordinated use of existing ones, such as HL7, DICOM, and FHIR through “profiles” that specify how systems should interact. These profiles enable interoperability between electronic health records, imaging systems, and other healthcare applications, ensuring consistent, secure, and efficient data exchange across organisations.
openEHR is an open standard and specification for managing electronic health records. It separates clinical knowledge from technical implementation using a two-level modeling approach: a stable reference model and flexible archetypes defined by clinicians. This allows systems to store, share, and interpret health data consistently over time. openEHR emphasises semantic interoperability, enabling different healthcare systems to understand and reuse clinical information accurately across organisations and applications.
Mind the gap
IHE primarily focuses on interoperability and the exchange of information between systems, rather than on how data is stored internally. IHE profiles define workflows, transactions, and communication patterns using standards like HL7 and DICOM, ensuring that systems can reliably share data. However, IHE provides little guidance on persistence mechanisms or detailed information models. Decisions about how data is structured, stored, and managed internally are left to individual implementations
And this is the gap: openEHR is fundamentally about defining a thorough information model that is reflected in persistence itself, not just in how data is exchanged. Relying on interoperability at the exchange layer alone risks losing the semantic richness that is of utmost importance in healthcare. Yet IHE has always been about that, which isn’t a weird thing, right? You can’t force healthcare vendors to conform to your idea of information model just to be able to exchange data. But it is where openEHR adds its true value and is an important aspect in the future health IT world we’re moving towards – a data-centric one, instead of a vendor-centric one, where interoperability is built in its core rather than an add-on.
The Plugathon
openEHR International and IHE set out to do a Plugathon in the Connectathon week in Brussels, with the idea of identifying potential collaboration opportunities and existing (or new?) IHE profiles where openEHR could be one of the standards. Immediate areas of exploration were MHD, mXDE and QEDm profiles and how they work with openEHR foundation underneath. We furthermore decided to focus on EHDS and IPS use cases to make it more tangible.
QEDm
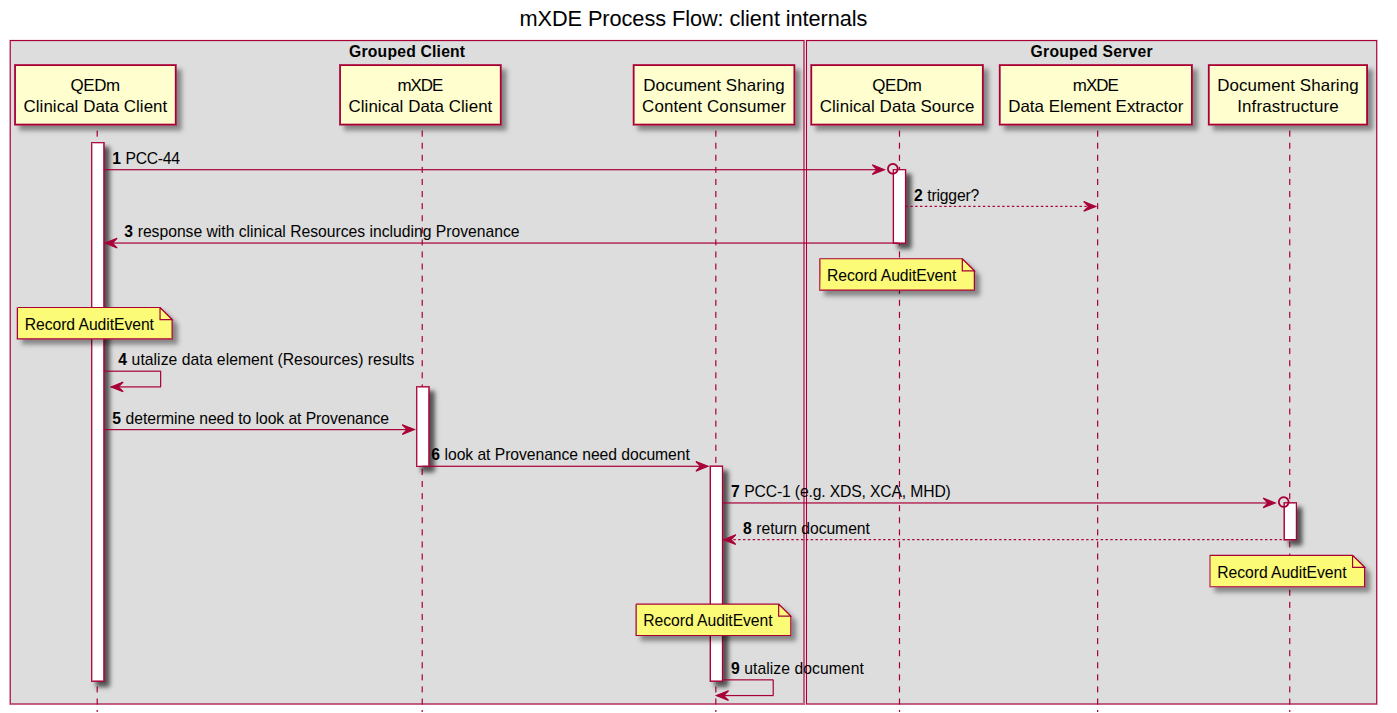
..stands for Query Existing Data (mobile – signaling that it follows a RESTful pattern). It describes the behavior of a client and a server-side component when one is querying for discrete data from (for example) an IPS section. Apart from describing the transactions, it furthermore describes how Provenance is tracked, what security considerations need to be obeyed, and what are the responsibilities of each actor. When one of the actors is an openEHR CDR (for server-side component), there are various details that could be specified, bringing the whole QEDm closer to openEHR stack and making it a standard actor grouping.
mXDE
…goes hand in hand with QEDm, because it’s all about how data is extracted from a structured data source (say: openEHR) and then exposed via QEDm. In the sequence diagram below, mXDE and “Document Sharing Infrastructure” would be a role for openEHR CDR bundled with a FHIRConnect engine (such as openFHIR). mXDE and QEDm profiles could further specify how the extraction and transactions look like when structured clinical content is openEHR. And a good first use case for this could be International Patient Summary (in EHDS landscape).
Live demo
IPS via openFHIR
See the mXDE / QEDm stack in action — International Patient Summary generated from an openEHR CDR using FHIRConnect and openFHIR.
Added value of openEHR
An obvious question out there is why openEHR and why would we try to bridge that gap between IHE and what is essentially a standard for persistence (simply put, I know it’s not really that). Why would IHE include this standard in one of those used in IHE profiles, if all that matters is exchange? QEDm is QEDm, it’s an exchange and defined in FHIR regardless of how data is actually represented at the source (in our case that would be openEHR), right?
That’s true.. to a point. And we could leave it at that, and openEHR could just be one of many data sources that has a FHIR facade on top, which is entirely possible now with a FHIRConnect standard. But the obvious added value of openEHR means that with it, you have a standard, reproducible and scalable stack based entirely on open standards. A vendor-neutral architecture where both information model and the exchange is standardised, community driven and interoperable out of the box, easily scalable in all possible dimensions – between vendors, between nations and furthermore easily scalable to other use cases. It’s no longer about adding an exchange layer and proprietary mapping of your data, but being interoperable at-source. Adding this whole stack to an IHE profile is no longer about putting a plaster on proprietary systems for the reason of exchange, but making a fundamental shift towards how open vendor-neutral systems should look like in the future (and can now, already).
There are many hospitals (..) that are looking at IHE compliance by vendors when choosing their system. And IHE compliance of a vendor is the next best thing, because it still promises some sort of interoperability and solution to a vendor lock-in, but it stops at that.. it stops at the bare minimum. What if there was an IHE profile completely mandating these three open standards (FHIR, FHIRConnect and openEHR) based on which vendors would 100% be able to deliver a vendor-neutral architecture, and not just a plug on the proprietary system, sufficing with the bare minimum to get the ribbon of being interoperable? Having that kind of ribbon as a vendor, and IHE proving that kind of capability is next level and would truly mean something to a hospital or a care provider.
Architecture
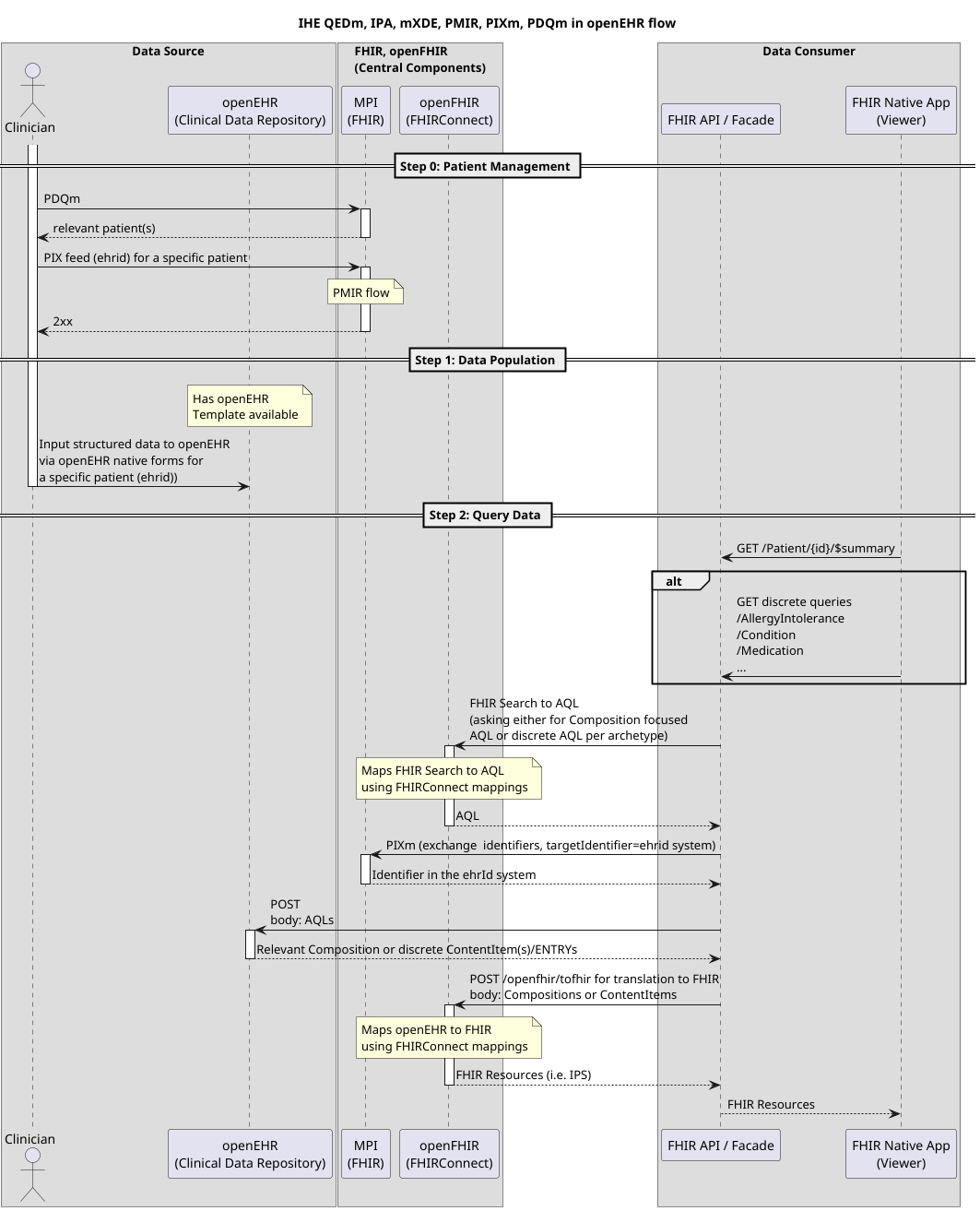
A couple levels deeper, this is how data flow would look like when openEHR acts as a Data Source in an architecture of IHE compliant actors (PIXm, PDQm, mXDE, QEDm, ..) that leverage FHIR. If you want to know more, feel free to ask Seref Arikan, PhD about an “EHR Slice“.
Key focus points
The plugathon was filled with discussion, but we always came back to what’s the first use case we’re trying to solve. What’s the first tangible problem that needs addressing? EHDS, IPS, and how the above profiles relate to them were our main focus points and the area of collaboration we plan to further deep dive into in upcoming newly established work group meetings.
But there is another idea: one where openEHR and FHIR together form a unique selling proposition for how forms are governed and used. It’s an idea that’s been ironed out in Igor Schoonbrood’s whitepaper on telemonitoring, providing deep insight into how openEHR’s strong data governance and forms bound to openEHR Templates work together with a FHIR SDC profile. openEHR fits this idea directly, while leveraging FHIR as an already established and widely adopted SDC profile; perhaps more so than trying to position openEHR within architectures like QEDm. A group of architects and experts, primarily in the Netherlands, has been brought together under Igor Schoonbrood’s leadership to evaluate the feasibility of this as an IHE profile.
Next steps
Having said that, there are more “focus” points where openEHR brings a lot to the table. But ultimately, this all circles back to the same idea: interoperability alone, especially when treated as an exchange layer, only gets us so far
What’s emerging from these discussions is not a challenge to IHE’s role, but an extension of it. If IHE has historically enabled systems to talk to each other, the next step could be enabling them to mean the same thing at their core. That’s where openEHR naturally fits in.
In that sense, the question is no longer just how systems exchange data, but what kind of architectures we want to standardise moving forward and whether interoperability should remain an add-on, or become intrinsic by design.
Gasper Andrejc is a Ljubljana-based Health IT professional and founder of openFHIR, specialising in FHIR architectures and backend reliability. He combines software engineering expertise with strong technical writing, improving clarity and reducing operational risk. His work spans APIs, integration workflows, and validation practices, with a focus on scalable, vendor-neutral systems that align interoperability with robust, future-ready data models.
Leave a Reply